Atypical genitalia, formerly termed ambiguous genitalia, is a rare condition observed at birth in which the external genitalia do not clearly resemble typical male or female anatomy. This condition results from disruptions during the fetal development of sex organs and hormones, leading to discrepancies between external genital appearance, internal sex organs, and genetic sex (chromosomal makeup).
Various criteria have been offered for the definition of intersex, including ambiguous genitalia, atypical genitalia, and differential sexual development. Ambiguous genitalia occurs in roughly 0.05% of all births, usually caused by masculinization or feminization during pregnancy, these conditions range from full androgen insensitivity syndrome to ovotesticular syndrome.
1.7% of people are born with a disorder of sexual development (DSD) as defined by the DSD consortium, such as those with Klinefelter’s syndrome. The DSD was specifically made to be as inclusive to all atypical sexual development; not all conditions within the DSD cause sexual ambiguity or affect individuals to the same extent. In other estimates, Definitions are limited to ambiguous conditions in which typical chromosomal categorization patterns is inconsistent with phenotypic sex, or in which the phenotype is not easily classifiable as either male or female,” with the prevalence of about 0.018%.
Most intersex activism is based around the end of unnecessary medical interventions on intersex youth which attempt to assign an arbitrary gender binary, often causing physical harm with no input from the child. Intersex conditions are usually expanded to include the DSD more generally, including conditions without sexual ambiguity. 0.05% of births are medically treated or considered to have ambiguous genitalia.
Key Characteristics
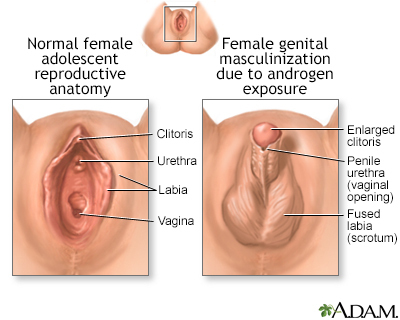
In Genetic Females (XX Chromosomes):
- Enlarged clitoris resembling a small penis.
- Closed or fused labia, which may look like a scrotum.
- Lumps in the labia, which could be undescended testicles.
In Genetic Males (XY Chromosomes):
- Hypospadias: The opening of the urethra is not at the tip of the penis but on its underside.
- Small penis (micropenis) with the urethral opening closer to the scrotum.
- Undescended testicles or an empty scrotum resembling labia.
Causes
Atypical genitalia arises from variations in the typical processes of sexual differentiation during fetal development. These may include:
- Hormonal Disruptions:
- Insufficient androgens in genetic males.
- Excess androgens in genetic females.
- Genetic Changes:
- Alterations in genes involved in sex organ development.
- Chromosomal abnormalities, such as missing or extra sex chromosomes.
- Medical Conditions:
- Congenital adrenal hyperplasia (CAH): Overproduction of androgens in genetic females.
- Androgen insensitivity syndrome: Tissues are unresponsive to androgens in genetic males.
- 5-alpha-reductase deficiency: A lack of enzymes required for male genital development.
- External Influences:
- Exposure to androgenic medications or hormone imbalances during pregnancy.
- Rare tumors in the pregnant individual producing masculinizing hormones.
Risk Factors
- Family History:
- Atypical genitalia or unexplained infant deaths.
- Infertility or unusual physical development during puberty.
- Congenital adrenal hyperplasia (CAH).
- Maternal Health:
- Exposure to certain medications or environmental toxins during pregnancy.
Complications
- Infertility: Some individuals may face challenges in conceiving depending on their specific condition.
- Increased Cancer Risk: Certain sex development differences are associated with higher risks of specific cancers, particularly of the gonads.
Management and Treatment
Diagnosis:
- Physical Examination: Evaluation of external genitalia.
- Imaging: Ultrasounds or MRIs to identify internal structures.
- Chromosomal Analysis: Determines genetic sex.
- Hormonal Testing: Evaluates levels and response to sex hormones.
Treatment Options:
- Hormonal Therapy:
- Administered to support typical development during puberty or later life.
- Surgical Intervention:
- Corrective surgeries may address functional or aesthetic concerns.
- Timing of surgery should consider potential psychological and physical impacts.
- Genetic Counseling:
- Helps families understand the condition and assess future risks.
Support for Families:
- Psychological Counseling: Aims to address emotional and social concerns for the child and family.
- Shared Decision-Making: Involves medical experts, psychologists, and families in determining the best care plan.
Conclusion
Atypical genitalia is not a disease but a variation in development requiring thoughtful medical and emotional support. Advances in medical care and personalized approaches enable individuals with this condition to lead healthy and fulfilling lives.
Many intersex activists have advocated for a spectrum based approach for intersex conditions, which would differentiate various intersex conditions, including hormonal differences. Intersex conditions, even the same conditions such as ovotesticular syndrome, can vary wildly in terms of organs, genetic expression, phenotype, genotype, and karyotype. Under this model intersex conditions would be described via their own individualized effects described as effecting individuals on a spectrum. The DSD generally describes this by the description of individualized care for people with atypical sexual development, making the distinction between different conditions.








{kind=link}